此次指南将STEMI和NSTE-ACS合并,开启了ACS诊疗指导新局面。
心血管疾病(CVD)是全球最常见的死亡和发病原因,急性冠脉综合征(ACS)通常是CVD的第一个临床表现,也是CVD最常见的死因[1]。2023年8月25日举行的欧洲心脏病学会年会(ESC 2023)重磅颁布了《2023 ESC ACS管理指南》,旨在为ACS患者的诊疗提供更为科学规范的指导。
 图 ESC 2023 ACS指南公布现场
图 ESC 2023 ACS指南公布现场
此次ACS指南提出了三个新概念:
表 2023版ACS管理指南更新要点
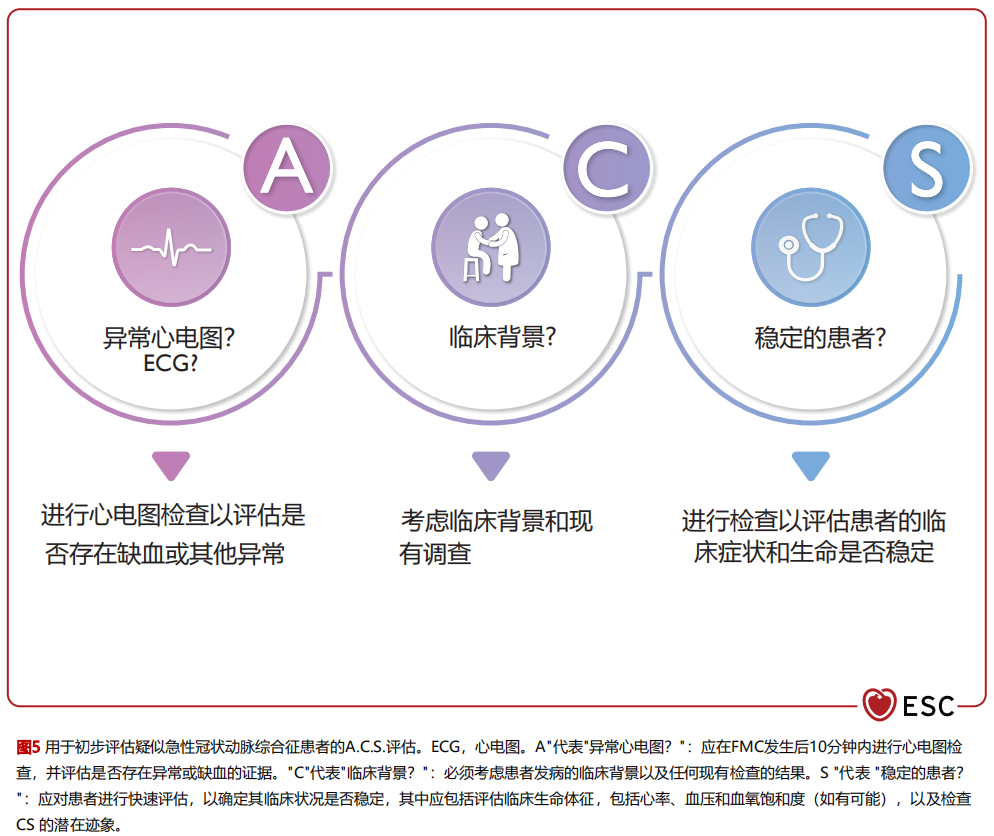
ACS包括一系列病症,其中包括近期临床症状或体征发生变化、12导联心电图有无变化、心肌肌钙蛋白有无急性变化的患者。新版指南提出用“A.C.S.方法”对疑似ACS患者进行初步评估,包括异常心电图abnormal ECG(A)、临床情况和病史Clinical context(C)、评估病情是否稳定Stable patient(S)。指南对于ACS患者的诊断及侵入策略评估有部分更新。
在ACS诊断方法方面,生物标志物高敏心肌肌钙蛋白(hs-cTn)仍然是诊断ACS重要的金标准,对于NSTEMI患者推荐采用0/1h或者0/2h进行快速Rule-in/Rule-out快速诊断(I类推荐)。而在影像学诊断方面,CT通常是排除其他可能危及生命的ACS鉴别诊断的诊断工具。但基于新进研究结果[2],对疑似NSTE-ACS的患者行早期无创的冠状动脉计算机断层扫描血管造影(CCTA)并不能改善其1年后的临床预后,因此指南进行更新,不推荐将CCTA作为疑似NSTE-ACS患者的一线影像检查方式(IIa类推荐)。
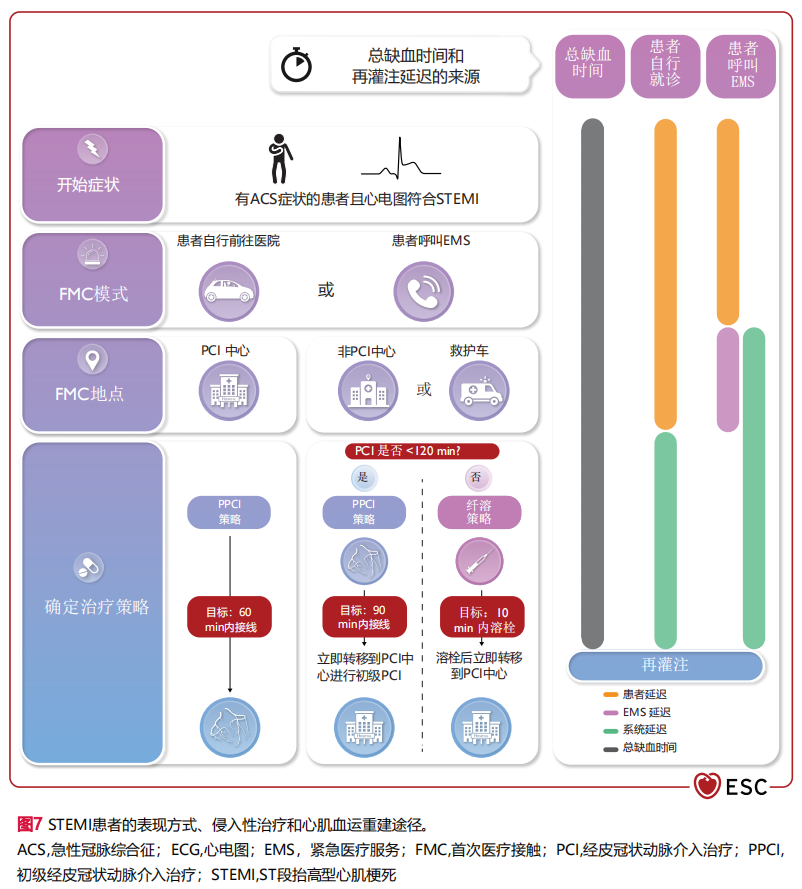
指南在侵入性策略方面同样有更新。对于STEMI患者,和既往推荐一致,建议应立即再灌注治疗[即直接经皮冠状动脉介入术(PPCI)策略或纤维蛋白溶解(如果在诊断后120分钟内无法进行PPCI)](I类推荐)。而对于NSTE-ACS的患者需进一步判定:当出现任何极高风险标准时,建议立即采取侵入性策略(I类推荐);当出现任何高风险标准时,建议在住院期间采用侵入策略(I类推荐),应考虑早期(即24小时内)侵入策略(IIa类推荐)。而在此前,对于24小时内的早期侵入策略推荐级别是I类推荐,此次推荐级别降低可能与多项荟萃分析[3-5]的阴性结果相关。
抗栓治疗是ACS患者治疗的重要组成部分。治疗的启用时机、药物选择及疗程制定取决于患者和手术等综合因素,须权衡抗血栓治疗的获益与出血风险[6-7]。
对于抗血小板治疗的药物推荐,和之前指南版本一致,基于PLATO研究[8]及TRITON-TIMI 38研究[9]结果,指南建议将包括阿司匹林和高效 P2Y12受体抑制剂[替格瑞洛或普拉格雷(未在中国获批)]在内的双联抗血小板疗法(DAPT)作为ACS患者的首选DAPT策略(I类推荐)。
氯吡格雷的特点是血小板抑制效果较差且不稳定,指南明确提出只有在替格瑞洛/普拉格雷有禁忌症或无法获取时,才能在某些高出血风险患者中使用。此外,指南提出对于部分老年患者,可考虑使用氯吡格雷,但值得注意的是此推荐级别仅为IIb,即可以使用但并不推荐[10-13]。
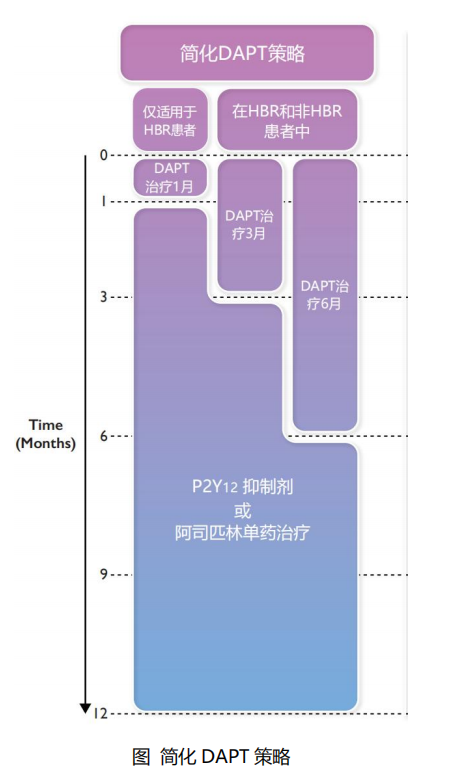
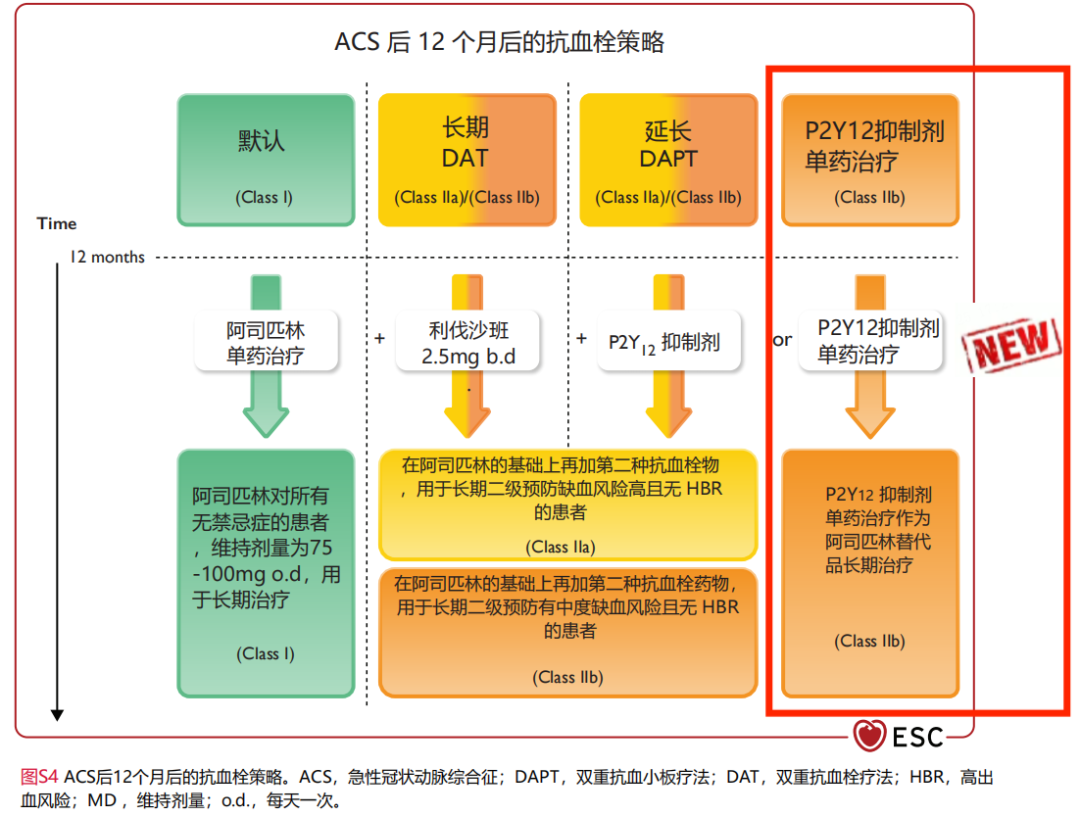
此外,对于ACS患者的疗程推荐,指南进行了“大刀阔斧”的更新:
对于3-6个月后无事件发生且缺血风险不高的患者可考虑单抗治疗,并优先P2Y12受体抑制剂(IIa类推荐)
在长期治疗中,可考虑将 P2Y12受体抑制剂单药治疗作为阿司匹林单药治疗的替代方案(IIb类推荐)
对于HBR 患者,可考虑在DAPT使用1个月后使用阿司匹林或P2Y12受体抑制剂单药治疗(IIb类推荐)
不推荐在发生ACS 事件后的前30天内降低抗血小板治疗的强度(III类推荐)
指南首次明确提出缩短DAPT后单抗药物更优先推荐P2Y12受体抑制剂而不是阿司匹林。既往部分研究[14-17]显示,在缩短DAPT治疗后继之以阿司匹林单抗方案中,出血事件的减少是以缺血事件的增加为代价。
而与之不同的是,P2Y12受体抑制剂单抗的明确获益,许多大型[18-21]随机对照试验探索DAPT时长缩短至1-3个月继之以P2Y12 受体抑制剂单抗治疗的优效性,如TWILIGHT研究[21-22](其中4,614例NSTE-ACS患者)结果证实DAPT 3个月后替格瑞洛单抗治疗能显著减少出血事件(BARC 2、3或5型出血),且未增加缺血风险。
与之结果类似的是,TICO研究[23](其中3056名ACS患者,36% STEMI)证实DAPT 3个月后采用替格瑞洛单抗治疗,净不良临床事件和主要出血事件明显减少,主要心血管不良事件(MACE)则无明显差异。但反之,STOPDAPT-2-ACS研究[24]结果并未得到证实,在ACS患者中缩短DAPT(<3个月)后氯吡格雷单药治疗或许并不是可行的策略。
值得注意的是,12个月DAPT(首选替格瑞洛/普拉格雷)仍然是ACS患者的默认策略,缩短策略作为替代方案通常是出于降低出血事件风险的动机。
此外,对于长期抗血小板治疗指南首次提出可考虑将 P2Y12受体抑制制剂单药治疗作为阿司匹林单药治疗的替代方案,此项推荐是基于HOST-EXAM研究[25]和一项评估ASCVD患者使用阿司匹林或P2Y12受体抑制剂(含15%噻氯吡啶、48%氯吡格雷、37%替格瑞洛)进行二级预防效果的荟萃分析[26]的结果。未来ACS患者对于长期单药抗血小板治疗的可选择性大大增加。
每位ACS患者都应尽早进行充分的二级预防,完善心脏康复、生活方式管理和药物治疗,以提高生活质量和降低发病率及死亡率。对此,指南也在血脂管理、血糖管理等方面也进行了更积极的治疗推荐。
低密度脂蛋白胆固醇(LDL-C)和ASCVD事件是因果关系,ACS事件发生后应尽早开始降脂治疗,以增加依从性及改善预后。指南提出在入院后尽早在经皮冠状动脉介入术(PCI)之前开始使用高强度他汀类药物(如瑞舒伐他汀),以最大耐受剂量达到LDL-C目标[27-28]。对于入院前正在接受降脂治疗的ACS患者,指南推荐在住院期间加强降脂治疗(I类推荐)。同时建议LDL-C目标值<1.4 mmol/L(<55mg/dL),并将LDL-C从基线降低≥ 50%(I类推荐)。
患有糖尿病的ACS患者更常出现非特异性症状及合并更多危险因素,这可能导致诊断和治疗延误、长期预后更差。考虑到ACS患者本身可能由于儿茶酚胺诱导的应激而引起高血糖,住院期间若新诊断糖尿病应后续随访观察。指南推荐对于所有ACS 患者,无论是否有糖尿病史,都应在住院期间对其血糖状况进行评估(I类推荐)。同时建议根据是否存在合并症(包括心衰、慢性肾脏病和肥胖)来选择长期降糖治疗方案(I类推荐)。
《2023 ESC ACS指南》开启了ACS诊疗指导新局面,基于最新的循证医学证据提出新的建议,其中包含药物治疗在内的综合管理仍是ACS管理的重中之重,此外更加强调患者的中心地位,旨在为患者提供更好的诊疗指导。
附:


[1]Roe MT,Harrington RA,Prosper DM,Pieper KS,Bhatt DL,Lincoff AM,et al.Clinicaland therapeutic profile of patients presenting with acute coronary syndromes who donot have significant coronary artery disease.Circulation 2000;102:1101–1106.[2]Ghadri JR,Wittstein IS,Prasad A,Sharkey S,Dote K,Akashi YJ,et al.International expert consensus document on Takotsubo syndrome(part II):diagnostic workup,outcome,and management.Eur Heart J 2018;39:2047–2062.[3]Navarese EP,Gurbel PA,Andreotti F,Tantry U,Jeong Y-H,Kozinski M,et al.Optimal timing of coronary invasive strategy in non-ST-segment elevation acute coronary syndromes:a systematic review and meta-analysis.Ann Intern Med 2013;158:261–270.[4]Jobs A,Mehta SR,Montalescot G,Vicaut E,van’t Hof AWJ,Badings EA,et al.Optimal timing of an invasive strategy in patients with non-ST-elevation acute coronary syndrome:a meta-analysis of randomised trials.Lancet 2017;390:737–746.[5]Kite TA,Kurmani SA,Bountziouka V,Cooper NJ,Lock ST,Gale CP,et al.Timing of invasive strategy in non-ST-elevation acute coronary syndrome:a meta-analysis of randomized controlled trials.Eur Heart J 2022;43:3148–3161.[6]Ali ZA,Maehara A,Genereux P,Shlofmitz RA,Fabbiocchi F,Nazif TM,et al.Optical coherence tomography compared with intravascular ultrasound and with angiography to guide coronary stent implantation(ILUMIEN III:OPTIMIZE PCI):a randomised controlled trial.Lancet 2016;388:2618–2628.[7]Ali ZA,Karimi Galougahi K,Maehara A,Shlofmitz RA,Fabbiocchi F,Guagliumi G,et al.Outcomes of optical coherence tomography compared with intravascular ultrasound and with angiography to guide coronary stent implantation:one-year results from the ILUMIEN III:OPTIMIZE PCI trial.Eurointervention 2021;16:1085–1091.[8]Wallentin L,Becker RC,Budaj A,Cannon CP,Emanuelsson H,Held C,et al.Ticagrelor versus clopidogrel in patients with acute coronary syndromes.N Engl J Med 2009;361:1045–1057.[9]van Leeuwen MAH,van der Hoeven NW,Janssens GN,Everaars H,Nap A,Lemkes JS,et al.Evaluation of microvascular injury in revascularized patients with ST-segment-elevation myocardial infarction treated with ticagrelor versus prasugrel.Circulation 2019;139:636–646.[10]Urban P,Mehran R,Colleran R,Angiolillo DJ,Byrne RA,Capodanno D,et al.Defining high bleeding risk in patients undergoing percutaneous coronary intervention:a consensus document from the Academic Research Consortium for High Bleeding Risk.Eur Heart J 2019;40:2632–2653.[11]Aradi D,Kirtane A,Bonello L,Gurbel PA,Tantry US,Huber K,et al.Bleeding and stent thrombosis on P2Y12-inhibitors:collaborative analysis on the role of platelet reactivity for risk stratification after percutaneous coronary intervention.Eur Heart J 2015;36:1762–1771.[12]Aradi D,Storey RF,Komócsi A,Trenk D,Gulba D,Kiss RG,et al.Expert position paper on the role of platelet function testing in patients undergoing percutaneous coronary intervention.Eur Heart J 2014;35:209–215.[13]Gimbel M,Qaderdan K,Willemsen L,Hermanides R,Bergmeijer T,de Vrey E,et al.Clopidogrel versus ticagrelor or prasugrel in patients aged 70 years or older with non-ST-elevation acute coronary syndrome(POPular AGE):the randomised,openlabel,non-inferiority trial.Lancet 2020;395:1374–1381.[14]Palmerini T,Della Riva D,Benedetto U,Bacchi Reggiani L,Feres F,Abizaid A,et al.Three,six,or twelve months of dual antiplatelet therapy after DES implantation in patients with or without acute coronary syndromes:an individual patient data pairwise and network meta-analysis of six randomized trials and 11 473 patients.Eur Heart J 2017;38:1034–1043.[15]Hahn J-Y,Song YB,Oh J-H,Cho D-K,Lee JB,Doh J-H,et al.6-month versus 12-month or longer dual antiplatelet therapy after percutaneous coronary intervention in patients with acute coronary syndrome(SMART-DATE):a randomised,open-label,noninferioritynoninferiority trial.Lancet 2018;391:1274–1284.[16]Kedhi E,Fabris E,van der Ent M,Buszman P,von Birgelen C,Roolvink V,et al.Six months versus 12 months dual antiplatelet therapy after drug-eluting stent implantation in ST-elevation myocardial infarction(DAPT-STEMI):randomised,multicentre,non-inferiority trial.BMJ 2018;363:k3793.[17]De Luca G,Damen SA,Camaro C,Benit E,Verdoia M,Rasoul S,et al.Final results of the randomised evaluation of short-term dual antiplatelet therapy in patients with acute coronary syndrome treated with a new-generation stent(REDUCE trial).EuroIntervention 2019;15:e990–e998.[18]Hahn J-Y,Song YB,Oh J-H,Chun WJ,Park YH,Jang WJ,et al.Effect of P2Y12 inhibitor monotherapy vs dual antiplatelet therapy on cardiovascular events in patients undergoing percutaneous coronary intervention:the SMART-CHOICE randomized clinical trial.JAMA 2019;321:2428–2437.[19]Vranckx P,Valgimigli M,Jüni P,Hamm C,Steg PG,Heg D,et al.Ticagrelor plus aspirin for 1 month,followed by ticagrelor monotherapy for 23 months vs aspirin plus clopidogrel or ticagrelor for 12 months,followed by aspirin monotherapy for 12 months after implantation of a drug-eluting stent:a multicentre,open-label,randomised superiority trial.Lancet 2018;392:940–949.[20]Watanabe H,Domei T,Morimoto T,Natsuaki M,Shiomi H,Toyota T,et al.Effect of 1-month dual antiplatelet therapy followed by clopidogrel vs 12-month dual antiplatelet therapy on cardiovascular and bleeding events in patients receiving PCI:the STOPDAPT-2 randomized clinical trial.JAMA 2019;321:2414–2427.[21]Mehran R,Baber U,Sharma SK,Cohen DJ,Angiolillo DJ,Briguori C,et al.Ticagrelor with or without aspirin in high-risk patients after PCI.N Engl J Med 2019;381:2032–2042.[22]Baber U,Dangas G,Angiolillo DJ,Cohen DJ,Sharma SK,Nicolas J,et al.Ticagrelor alone vs.ticagrelor plus aspirin following percutaneous coronary intervention in patients with non-ST-segment elevation acute coronary syndromes:TWILIGHT-ACS.Eur Heart J 2020;41:3533–3545.[23]Kim BK,Hong SJ,Cho YH,Yun KHo,Kim YH,Suh Y,et al.Effect of ticagrelor monotherapy vs ticagrelor with aspirin on major bleeding and cardiovascular events in patients with acute coronary syndrome:the TICO randomized clinical trial.JAMA 2020;323:2407–2416.[24]Watanabe H,Morimoto T,Natsuaki M,Yamamoto K,Obayashi Y,Ogita M,et al.Comparison of clopidogrel monotherapy after 1 to 2 months of dual antiplatelet therapy with 12 months of dual antiplatelet therapy in patients with acute coronary syndrome:the STOPDAPT-2 ACS randomized clinical trial.JAMA Cardiol 2022;7:407–417.[25]Koo BK,Kang J,Park KW,Rhee T-M,Yang H-M,Won KB,et al.Aspirin versus clopidogrel for chronic maintenance monotherapy after percutaneous coronary intervention(HOST-EXAM):an investigator-initiated,prospective,randomised,open-label,multicentre trial.Lancet 2021;397:2487–2496.[26]Chiarito M,Sanz-Sánchez J,Cannata F,Cao D,Sturla M,Panico C,et al.Monotherapy with a P2Y(12)inhibitor or aspirin for secondary prevention in patients with established atherosclerosis:a systematic review and meta-analysis.Lancet 2020;395:1487–1495.[27]Mach F,Baigent C,Catapano AL,Koskinas KC,Casula M,Badimon L,et al.2019 ESC/EAS Guidelines for the management of dyslipidaemias:lipid modification to reduce cardiovascular risk.Eur Heart J 2020;41:111–188.[28]Navarese EP,Kowalewski M,Andreotti F,van Wely M,Camaro C,Kolodziejczak M,et al.Meta-analysis of time-related benefits of statin therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention.Am J Cardiol 2014;113:1753–1764.*"医学界"力求所发表内容专业、可靠,但不对内容的准确性做出承诺;请相关各方在采用或以此作为决策依据时另行核查。